Assessing the respiratory system can seem like a daunting task, but it’s a critical component of any health assessment. Whether you're a healthcare professional or simply someone who wants to ensure they're taking proactive steps towards better health, understanding the fundamentals of respiratory assessment is crucial. This guide will walk you through everything you need to know about evaluating the respiratory system effectively and accurately. We’ll start by addressing the common problems users face and then delve into practical solutions with a problem-solving focus, ensuring you gain the knowledge to perform these assessments confidently.
Understanding Common Respiratory Assessment Challenges
Recognizing the intricacies of respiratory health assessments can be challenging for many. Common issues include difficulty in accurately assessing breath sounds, uncertainty in distinguishing between normal and abnormal findings, and a lack of confidence in diagnosing subtle abnormalities. Many also struggle with identifying which symptoms could indicate a more serious underlying condition. This guide aims to address these pain points, offering step-by-step guidance that is both practical and actionable, ensuring you can accurately and confidently perform these evaluations.
Quick Reference
- Immediate action item: Always start with a visual inspection, noting any signs of distress.
- Essential tip: Use a stethoscope to listen for clear and distinct breath sounds in all lung fields.
- Common mistake to avoid: Failing to properly clean and cap the stethoscope after each use to prevent the spread of infection.
How to Conduct a Respiratory System Assessment
A thorough respiratory system assessment is crucial for detecting and diagnosing respiratory disorders. Here’s a step-by-step guide to conducting a comprehensive assessment:
Step 1: Preparation
Before beginning the assessment, ensure that the environment is calm and quiet, and that you have all necessary tools: a stethoscope, a thermometer, a sphygmomanometer, and a notepad to record findings. Make sure the patient is comfortably seated or lying down.
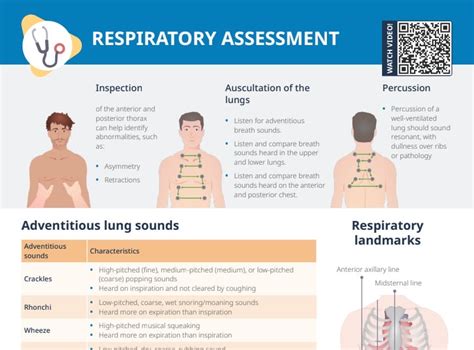
Step 2: Visual Inspection
Start with a visual inspection of the patient’s overall appearance and chest movement.
- Note any signs of respiratory distress, such as rapid breathing, nasal flaring, or use of accessory muscles.
- Observe for chest asymmetry, which could indicate a pneumothorax or pleural effusion.
Step 3: Palpation
Use your hands to palpate the chest for symmetry and to assess for tenderness or subcutaneous air.
- Check for any abnormal vibrations or crepitus, which might indicate lung consolidation or subcutaneous emphysema.
Step 4: Percussion
Begin percussion over the anterior chest to identify areas of dullness or hyperresonance.
- Percuss across the entire chest surface to map out the boundaries of the heart, liver, and lungs.
Step 5: Auscultation
This is the most critical part of the assessment, where you will listen to the patient’s breath sounds.
Here’s a step-by-step breakdown:
- Place the diaphragm of the stethoscope at the second intercostal space at the right midclavicular line and listen for normal breath sounds.
- Repeat the process systematically across all lung fields, including the anterior, lateral, and posterior chest.
- Listen for adventitious sounds such as wheezes, rales, and rhonchi, which could indicate different respiratory pathologies.
Step 6: Additional Assessments
Consider other tests based on initial findings:
- Pulse oximetry to measure oxygen saturation levels.
- Peak flow meter tests for assessing lung function in patients with known asthma or COPD.
- Blood gas analysis for severe respiratory distress cases.
Practical Examples and Case Studies
To make the learning process more tangible, here are some practical examples and case studies.
Example 1: Identifying Pneumonia Symptoms
Patient presents with a cough, fever, and reports feeling generally unwell.
- During auscultation, you hear bronchial breath sounds and crackles in the lower lobes.
- Additional percussion reveals dullness over the affected area.
These findings, combined with the patient’s symptoms, strongly suggest a diagnosis of pneumonia.
Example 2: Differentiating Between Asthma and COPD
Patient has a history of recurrent wheezing and dyspnea.
- Auscultation reveals expiratory wheezes, which are more pronounced after exertion.
- You also notice prolonged expiration and reduced airflow.
These characteristics are typical of chronic obstructive pulmonary disease (COPD), but it’s essential to differentiate from asthma, often by noting the response to bronchodilators.
What should I do if I find abnormal breath sounds?
If you detect abnormal breath sounds such as wheezes, crackles, or decreased breath sounds, it's critical to further investigate these findings:
- Document the specific locations and types of abnormal sounds.
- Perform additional diagnostic tests, like chest X-rays or CT scans, as indicated.
- Consult with a pulmonologist for a comprehensive evaluation and appropriate management.
Always follow up with the patient to monitor any changes in symptoms or findings.
Best Practices and Tips
Here are some best practices and tips to enhance the accuracy and effectiveness of your respiratory assessments:
- Maintain good hygiene by cleaning the stethoscope between patients to prevent cross-contamination.
- Use proper techniques for auscultation, including listening in a quiet environment and applying moderate pressure with the diaphragm.
- Continuously update your knowledge through training and staying informed about the latest developments in respiratory health.
Remember, a thorough respiratory assessment not only helps in diagnosing various respiratory conditions but also contributes significantly to patient care and outcomes. By following the steps and guidelines provided in this guide, you can perform accurate and effective respiratory system assessments, addressing the essential needs of your patients.


